- other parts of the jaw or the ilium (pelvic area) of the same patient (auto-grafts)
- another donor’s bone, which has undergone specific treatment and sterilization procedures (allo-grafts)
- an animal’s bone material, usually from cattles or pigs, that have undergone specific treatment and sterilization procedures (xeno-grafts)
- synthetic material (alloplastic implants)
- bone morphogenetic proteins and growth factors
Except auto-grafts, all other types of grafts are available in the market. Due to their processing and the scrutinous assessment of quality control, they are totally safe for the patient. Usually, they are in a dried status, in the form of small granules, which, when dissolved in saline water, turn into a putty compound. In some other cases they come in a gel form.
Membranes are bio-materials that are used for the isolation and protection of the bone graft from the gingiva (gums). They can be absorbable (made of collagen or pericardium) or non-absorbable (made of Gore-Tex). Depending on the case, the appropriate type of membrane that will be used is chosen. In some bone grafts, however, the use of a membrane is not obligatory.
-

- Bone graft in granule form (Bio-Oss)
-

- Bone graft in gel form (Emdogain)
-

- Absorbable collagen membrane (Bio-Gide)
- in the formation of new supportive bone around a tooth that has lost bone due to periodontitis (guided tissue regeneration)
- in the preservation of the dimensions of the jaw bone after tooth extraction (socket preservation)
- in the maxillary sinus elevation
- in the increase of the dimensions of the bone, in deficient areas of the jaw (ridge augmentation)
The most common uses of a bone graft are socket preservation and ridge augmentation in order to obtain enough bone volume to place implants. The bone grafts, depending on the case, can be simultaneously placed with the dental implants, thus reducing the treatment period or the number of surgical sessions.
This process is called Guided Tissue Regeneration. The bone graft is surgically placed under local anesthesia and after the plaque has been removed. Typically, over the bone graft a special absorbable membrane is placed in order to protect the graft. Radiographically the new bone is visible after about six months.
-

- Initially
-
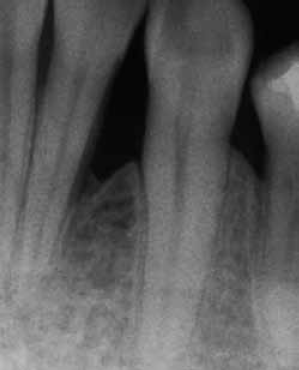
- After 12 months (Emdogain)
-
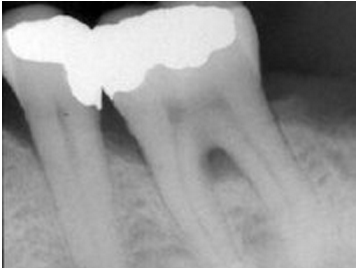
- Initially
-
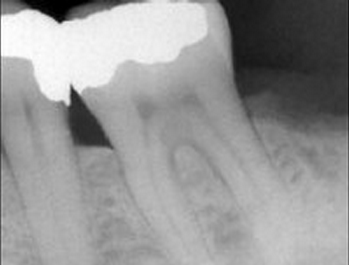
- After 12 months (Emdogain)

 Normal resorption of the jaw bone after tooth extraction
Normal resorption of the jaw bone after tooth extraction
In order to avoid such unpleasant situations, after the atraumatic extraction of a tooth the socket is filled with a bone graft material. This graft will minimize bone resorption and will facilitate the formation of new bone in the socket.
 Socket preservation
Socket preservation

If the distance from the ridge of the jaw until the maxillary sinus is big enough, then an implant can be placed.

Sometimes, though, after the extraction of a posterior tooth, the sinus begins to move downwards due to the absence of the tooth root. Hence, the sinus starts occupying the space of the jaw where the root was. Thus, the placement of an implant in this region may not be possible, because the penetration of the sinus by the implant is not desirable.


To resolve this problem, we resort to a surgical procedure called maxillary sinus elevation. During this surgery, the periodontist, after having gained access to the maxillary sinus, moves it upwards and fills the empty space with a bone graft. Thus, new bone is formed again in the region and the implant can now be placed. The elevation of the maxillary sinus is done under local anaesthesia. The minor discomfort that the patient may experience post-surgically is treated with mild pain killers.





In these cases, the reconstruction of the jaw bone with bone grafts is necessary prior to implant placement. It is reasonable, that the more extensive the defect the more challenging the grafting procedure may become.








